

How Bad is My Child's Myopia?

Author: Jason Higginbotham
BSc (Hons) MCOptom Prof Cert Glau Prof Cert Med Ret Prof Cert LV FBDO MBCLA
How Bad is my Child's Myopia?
It’s one of the first questions parents ask after hearing the word myopia. You’re given a number — maybe -1.50, -3.00 or even -6.00 — and naturally you wonder: Is this serious? Is it going to get worse? Should I be worried?
The truth is that myopia isn’t just about how blurry things look without glasses. While stronger prescriptions can certainly be frustrating in daily life, the more important issue is what that number represents — eye growth. Myopia usually develops because the eye grows longer than it should, and that elongation is what can increase the risk of eye health problems later in life if progression continues unchecked.
The good news is that not all myopia is the same, and not every child faces the same level of risk. How old your child is, how quickly their prescription is changing, and how long their eyes are (axial length) all matter.
This guide will help you understand what different prescription ranges mean, when myopia is simply inconvenient, when it deserves closer monitoring, and why managing progression early can make a meaningful difference to long-term eye health.
Is My Child's Prescription Bad?
It’s one of the most common questions parents and young adults ask: “Is -1.50 bad?” “Is -4.00 really bad?” “What does -6.00 actually mean?” The honest answer is that a prescription number on its own doesn’t tell the whole story - but it does give important clues.
Understanding What the Number Means
A minus prescription (for example, -2.00 or -5.00) means myopia, or short-sightedness. The higher the minus number, the stronger the lens needed to focus clearly at distance. Clinically, myopia is often grouped as:
-
Low myopia: around -0.50 to -3.00
-
Moderate myopia: -3.00 to -6.00
-
High myopia: greater than -6.00
From a day-to-day perspective, even low myopia can mean blurred classroom boards, road signs, or sports performance without glasses. But from a health perspective, the more important issue is not simply how blurry things are — it’s how the eye is growing.

Why “How Bad Is It?” Is the Wrong Question
A better question than “Is my child's prescription bad?” is:
“Is my child's myopia progressing, and what does that mean long term?”
Myopia usually develops because the eye grows too long (increased axial length). As the eye elongates, the delicate tissues at the back of the eye stretch. Over many years, this stretching increases the lifetime risk of conditions such as retinal detachment, myopic maculopathy, glaucoma and cataracts.
The Hidden Factor: Axial Length
Most people are only told their prescription. Far fewer are told their axial length — the actual physical length of the eye.
Two children might both be -3.00 today. One may have stable eye growth. The other may be progressing rapidly and on a path towards high myopia. Without tracking axial length over time, it’s difficult to see that difference.This is why monitoring growth matters. It shifts the focus from reacting to stronger glasses to understanding what is happening structurally inside the eye.
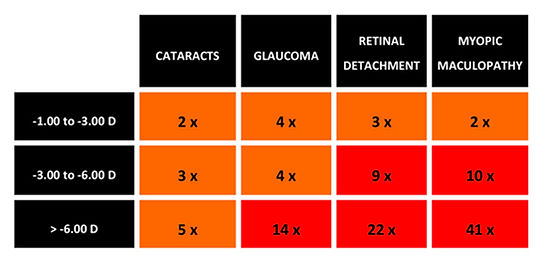
This table shows the increased risk of cataract, glaucoma, retinal detachment and myopic maculopathy (which is essentially a form of macular degeneration).
As the chart shows, the risks rise significantly with higher levels of myopia. Someone with high myopia does not just have stronger glasses — they may also have a meaningfully higher risk of future eye disease compared to someone with low myopia.
That doesn’t mean problems are inevitable. It means that risk increases with degree of elongation, particularly if myopia progresses unchecked during childhood.
FOCUS
POINT
Myopia typically develops in childhood as a result of the eye growing too long from front to back which is referred to as the axial length of the eye
So, Is your Child's prescription bad?
And more importantly - is my child's prescription bad for me to take action? And what action should I take? The best advice - as always - is to find and speak to a local myopia specialist near you, but, here's another attempt to help you understand. The impact of myopia depends on four things:
-
How strong the prescription is (dioptres)
-
How long your axial length is
-
How old you are and,
-
Whether your 'myopia' it’s still progressing - your axial length is growing on your dioptre is getting worse!
Blurry vision is frustrating. But the real long-term concern isn’t blur — it’s eye elongation (axial length). That’s what increases lifetime risk.
Here’s how different ranges typically compare.
0.00 to -1.00 D – Very Mild Myopia
At this level, distance vision is slightly blurred, especially:
-
Classroom boards
-
Road signs
-
Sports played at distance
-
Watching TV across the room
Some children may only need glasses part-time.
From a health perspective, this level of myopia is common and usually low risk if it remains stable. The key question is not “Is this bad?” but:
Is it the beginning of progression?
If a 7-year-old is already -1.00, monitoring becomes important. If a 17-year-old is -1.00 and stable, risk is much lower.
-1.00 to -3.00 D – Low Myopia
This is where daily life becomes more affected without correction:
-
Sports performance can suffer
-
Swimming without prescription goggles becomes difficult
-
Recognising faces at distance is harder
-
School performance may be impacted if uncorrected
-
At this stage, vision correction works very well. With glasses or contact lenses, most people see clearly.
Long-term health risk is still relatively low — if progression slows or stops.
But in younger children, this range often represents the start of a growth pattern. The concern isn’t being -2.00 today. The concern is whether that child becomes -6.00 or -8.00 later.
-3.00 to -6.00 D – Moderate Myopia
This is where myopia becomes more significant.
Without glasses, distance vision is very blurred. Daily life without correction becomes difficult. Many children in this range are progressing.
From a health perspective, risk begins to rise more noticeably here. The eye is typically longer than average, and the stretching of the retina increases lifetime risk of:
-
Retinal detachment
-
Glaucoma
-
Myopic maculopathy
-
Earlier cataracts
It’s important to stress: these conditions are not inevitable. But statistically, risk increases as axial length increases.
This is often the stage where myopia management strategies are most relevant.
-6.00 to -10.00 D – High Myopia
This is considered high myopia.
Vision without correction is extremely blurred. Daily functioning depends heavily on glasses or contact lenses.
More importantly, axial length is usually significantly above average. At this level:
-
Lifetime risk of retinal complications rises meaningfully
-
Myopic maculopathy becomes a concern
-
Monitoring by an eye care professional is essential
Again, the issue isn’t the inconvenience of thick lenses. It’s structural stretching of the eye over time.
Stopping progression before reaching this level is why early management matters.
-10.00 D and Beyond – Very High / Pathological Myopia
This level is uncommon but does occur.
Axial length at this stage is typically very long. Risks increase substantially, particularly for:
-
Retinal detachment
-
Degenerative retinal changes
-
Vision-threatening maculopathy
Regular specialist monitoring is essential.
The good news is that modern myopia management aims to reduce the number of children who ever reach this level.
The Bigger Picture: It’s About Growth, Not Just Blur
It’s easy to focus on how annoying blurry vision is — and it is annoying. Not seeing the board. Missing the football. Struggling in the swimming pool. But the real medical concern is not the blur, it’s how long the eye becomes over time.
Two children can both be -3.00. One may stabilise. The other may continue progressing into high myopia. The difference is often visible in axial length measurements, not just prescription changes.
That’s why tracking matters.
Age Matters
-
A 6-year-old at -2.00 is very different from
-
A 16-year-old at -2.00
Younger onset generally means more years of potential progression. Earlier progression increases the chance of higher final myopia.
So when asking, “Is my child's prescription bad?” the critical to also bear in mind their age and progression.
If your child has myopia:
-
Understand their prescription range
-
Ask about axial length measurement
-
Monitor progression over time
-
Explore management options if appropriate
You can also use our Myopia Visualiser to understand what different prescriptions look like in real life, and explore our guides on axial length, progression, and long-term risk.
Because the goal isn’t to panic about a number.
It’s to understand it — and act early if needed.